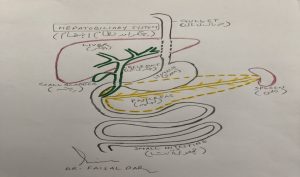
How the Bile Ducts work:
Bile a green-colored fluid produced by the liver cells. It collected within the bile ducts and transported to the gall bladder for storage. The bile from the liver mixes up with the food from the stomach and helps to absorb vitamins (like vitamin D and E) and required for the process of breaking down fats from our diet.
The presence of food within the first part of the small intestine (duodenum) stimulates the gall bladder to contract and squeeze bile out of the gall bladder, into the duodenum. Here it helps to digest and absorb the fats in the food.
Bile contains bile salts and bile pigments, most of which are recycled and the excessive ones are passed out of the body through urine and feces. The blockage of the bile duct system leads to dark urine and pale stools.
he human body made up of millions of cells. These cells different shapes and functions in different parts of the human body. The routine wear & tear of the body cells controlled by a process called the cell cycle. This process strictly regulated by the body’s control mechanisms. In cancers, the cells reproduce in an uncontrolled fashion which can lead to the formation of growth or tumor. The cancer cells develop the ability to invade and destroy surrounding cells by a process called invasion and eventually can spread to the other parts of the body (a process called metastases).
Some of the cells form a lump malignant (cancerous). others benign (non-cancerous). The cells which do not spread to other parts of the body (benign tumors) may cause symptoms as they grow by pressing on the surrounding organs. A lump diagnoses as benign or malignant with help of different investigations. such as blood tests, x-rays, ultrasound, and CT scans. Examination of the affected cells under a microscope can confirm the diagnosis of cancer. The special stains & techniques can also help to determine the origin of cancer.
Cholangiocarcinoma:
Cancer that starts anywhere within the biliary system called cholangiocarcinoma. “Cholangio” means bile duct and “carcinoma” means cancer. Bile duct cancer is a very uncommon cancer and not much known about its cause. The presence of choledochal (bile duct) cysts, primary sclerosing cholangitis (a disease of the bile ducts within the liver), and gallstones leading to chronic bile duct irritation associated with the increased incidence of bile duct cancer. Bile duct cancer usually a slow-growing cancer and can spread to other parts of the body in the later stages of the disease. Its incidence of about 20 per million population and affects both men and women equally. Usually, it more common in people over 65 years of age. however recently young patients in their 4th decade of life are being diagnosed with bile duct cancer in Pakistan.
Symptoms of Bile Duct Cancer:
The general symptoms are non-specific and include weight loss, lethargy/tiredness, loss of appetite, indigestion, and abdominal pain.
Once cancer causes a blockage of the bile ducts symptoms to include pale feces, dark urine, itching, and jaundice.
Clinical evaluation by the doctor to look for the presence of jaundice (yellowness of skin and eyes) or presence of scar marks (due to itching) and presence of any lumps in the tummy.
Blood tests including LFTs (bilirubin level in your blood high due to the blockage of the bile duct).
Hemoglobin (Hb level) can below
Tumor markers. These are substances normally seen in the blood, however, in people with cancer, they may be high. In bile duct cancer, the tumor marker associated with it is Ca19.9.
Ultrasound scan
CT scan
MRI (magnetic resonance imaging)
Endoscopic Retrograde Cholangio-Pancreatography (ERCP)
Endoscopic ultrasound (EUS)
You may undergo one or more of the scans in order to help identify the tumor and assess your suitability for the various treatments.
Histology/cytology:
All of the previously mentioned tests may lead the doctor to diagnose bile duct cancer. However, the only definite way to confirm this diagnosis is to examine some of the abnormal tissue (cancer cells) under a microscope. Some cells may be taken during the ERCP procedure (these are called brushings). These cells taken to the laboratory for cytology examination. However, the results of cytology do not always produce a diagnosis and may give a negative result, despite cancer existing. If a larger sample of tissue required we may perform a biopsy. This when a needle passed through your skin, into the affected area. If your doctor planning to treat your cancer with surgery, you may not undergo a biopsy, as tissue confirmation can obtain after the operation, by the laboratory.
Treatment:
Complete surgical removal of the cancer is the mainstay of bile duct cancer treatment. The aim of the treatment to treat cancer and any symptoms it may cause. Treatment of the bile duct cancer depends on the stage of cancer and may differ from person to person because of:
Location of Cancer:
The bile duct cancer can occur anywhere within the bile duct system. There bile ducts throughout the liver – these called intra (within) hepatic (liver) bile ducts. some of which may run alongside major vessels that supply blood to or return blood from the liver.
There are also bile ducts that run from the liver to the gall bladder, and then from the gall bladder to the duodenum – these called extra (outside) hepatic ducts.
Size of Cancer:
The bile duct cancers can grow to a relatively large size causing any symptoms. Some cancers too small to identify scanning tests.
The spread of Cancer:
CT scans can detect whether cancer spread to any other part of the body – including the lymph glands. As the lymph system runs throughout the body, cancer that may have spread to the lymph system can increase the risk of further cancer spread (metastases) or increase the risk of cancer recurrence where main cancer already surgically removed.
Age of the patient:
Age can affect how well your body works, however, when deciding on which treatment the best for each individual. it important to assess each person’s actual health, rather than expected health for someone of that age.
Associated medical problems:
Are you well despite having another illness or does you have other medical problem limiting your lifestyle or life expectancy? Curable or palliative (may alleviate symptoms) therapies may offer to you, depending on the factors mentioned above. The clinical team caring for you will discuss, with you, the different treatments and therapies available. They will assist and support you in making decisions and choices about what is right for you.
The prognosis (chance of recovery) and treatment options depend on the following:
- The stage and extent of cancer (whether it is in the stomach only or has spread to lymph nodes or other places in the body).
- The patient’s general health.
When gastric cancer is found very early, there is a better chance of recovery. Gastric cancer is often in an advanced stage when it is diagnosed. At later stages, gastric cancer can be treated but rarely can be cured.
Treatment options
There are different types of treatment for patients with gastric cancer. Different types of treatments are available for patients with gastric cancer. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. Before starting treatment, patients may want to think about taking part in a clinical trial. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment.
Four types of standard treatment are used:
Surgery: Surgery is a common treatment of all stages of gastric cancer. The following types of surgery may be used:
Subtotal gastrectomy – removal of the part of the stomach that contains cancer, nearby lymph nodes, and parts of other tissues and organs near the tumor. The spleen may be removed. The spleen is an organ in the upper abdomen that filters the blood and removes old blood cells.
Total gastrectomy – removal of the entire stomach, nearby lymph nodes, and parts of the esophagus, small intestine, and other tissues near the tumor. The spleen may be removed. The esophagus is connected to the small intestine so the patient can continue to eat and swallow.
If the tumor is blocking the stomach but cancer cannot be completely removed by standard surgery, the following procedures may be used:
Endoluminal stent placement – a procedure to insert a stent (a thin, expandable tube) in order to keep a passage (such as arteries or the esophagus) open. For tumors blocking the passage into or out of the stomach, surgery may be done to place a stent from the oesophagus to the stomach, or from the stomach to the small intestine to allow the patient to eat normally.
Endoluminal laser therapy – a procedure in which an endoscope (a thin, lighted tube) with a laser attached is inserted into the body. A laser is an intense beam of light that can be used as a knife.
Chemotherapy: Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the spinal column, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). The way the chemotherapy is given depends on the type and stage of the cancer being treated.
Radiation therapy: Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy. External radiation therapy uses a machine outside the body to send radiation toward cancer. Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near cancer. The way radiation therapy is given depends on the type and stage of the cancer being treated.
Chemoradiation: Chemoradiation combines chemotherapy and radiation therapy to increase the effects of both. Chemoradiation treatment given after surgery to increase the chances of a cure is called adjuvant therapy. If it is given before surgery, it is called neo-adjuvant therapy.
The outlook for stomach cancer depends on the stage of the cancer. People in the early stages of stomach cancer have a much greater rate of survival than those at a later stage:
- If stomach cancer is found in its earliest stage and can be removed with an endoscope, the five-year survival rate is higher than 90 percent.
- If the cancer is found after it has spread to areas surrounding the stomach, the five-year survival rate is 28 percent.
- If the cancer has spread to areas beyond those surrounding the stomach, the five-year survival rate is 4 percent.